Identifying an acute myocardial infarction on the 12-lead ECG is the most important thing you can learn in ECG interpretation.
Time is muscle when treating heart attacks. Missing a ST segment elevation MI on the ECG can lead to bad patient outcomes. It’s just not good. So let’s go over the ECG findings in STEMI — again, and again, and again — with multiple examples. This way, you can drill into your memory what each type of STEMI looks like on the 12-lead ECG.
There are five basic acute MI ECG patterns you will encounter. But sure, there are a few variations of each of these, and that is why looking at as many examples as possible is crucial — as mentioned in 10 Steps to Learn ECG Interpretation.
Type #1: Anterior ST Segment Elevation MI
This is the big one that carries a high mortality if not treated rapidly. An anterior STEMI is usually from acute thrombotic occlusion of the left anterior descending coronary artery — also known as the “widow maker.”
Recall that the anterior leads are technically V3 and V4; however, it is common for the septum and/or lateral wall to be involved during anterior MIs, as the LAD supplies septal branches to the interventricular septum and diagonal branches to the lateral wall. The septum is represented on the ECG by leads V1 and V2, whereas the lateral wall is represented by leads V5, V6, lead I and lead aVL. To make things more complicated, sometimes the LAD “wraps around” the cardiac apex, which is a common anatomic variant. This results in part of the inferior wall being supplied by the LAD, as well. Oh, my!
and/or lateral wall to be involved during anterior MIs, as the LAD supplies septal branches to the interventricular septum and diagonal branches to the lateral wall. The septum is represented on the ECG by leads V1 and V2, whereas the lateral wall is represented by leads V5, V6, lead I and lead aVL. To make things more complicated, sometimes the LAD “wraps around” the cardiac apex, which is a common anatomic variant. This results in part of the inferior wall being supplied by the LAD, as well. Oh, my!
We will get to the examples soon, but first we need to understand some more basics of anterior MIs.
If the thrombus is in the proximal LAD, the septum and lateral walls will often also be involved, in addition to the anterior segments, resulting in ST segment elevation in leads V1 through V6 and perhaps lead I and aVL, as well.
When the thrombus is in the mid LAD (after the septal branch), the diagonal branch(es) may or may not be involved. If this is the case, then the ST segment elevation will be in V3 to V6 — and not the septal leads.
Because the anatomical opposite of the precordial leads would be posterior leads, which we do not commonly check in this setting, there are no “reciprocal changes” during anterior or septal MIs. Now, “high lateral” MIs with ST segment elevation in the limb leads I and aVL can show reciprocal ST segment depression in leads II, III and aVF.
Here is some more terminology. When there is not only anterior ST segment elevation (V3 and V4), but also septal (V1 and V2) and lateral (V5, V6, lead I and lead aVL), an “extensive anterior” MI is said to be present.
Recall, as well, that a STEMI is a STEMI is a STEMI. Treatment for all of them is the same, regardless of what pattern it takes — that is quick coronary revascularization.
Lastly, the official definition of STEMI according to the American College of Cardiology/American Heart Association guidelines for STEMI is “new ST segment elevation at the J point in at least two contiguous leads of ≥ 2 mm (0.2 mV) in men or ≥ 1.5 mm (0.15 mV) in women in leads V2-V3 and/or of ≥ 1 mm (0.1 mV) in other contiguous chest leads or the limb leads.” This means 1 mm in any two contiguous leads except leads V2 or V3, where the elevation must be 2 mm in men or 1.5 mm in women.
Below are the anterior MI ECG patterns that you may encounter.

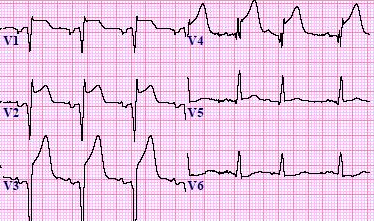
This is named for obvious reasons. The J point is elevated and, along with the T wave, and it looks like a tombstone. In an anterior MI that shows “tombstoning,” there is frequently 4 to 6 millimeter of ST segment elevation. Do not confuse the ST segment elevation with the T wave. Look specifically where the ST segment is — waaaaay up from the baseline. Recall that the J point is where we need to measure the elevation from baseline, and the baseline is always the TP segment (between the T wave and the P wave).
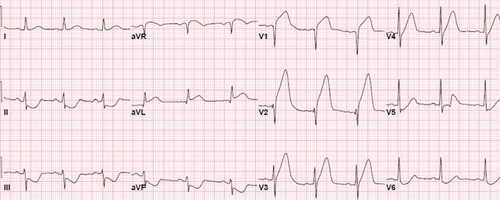
Below is another example of tombstoning with a slightly different shape. There is septal involvement (lead V2) and a bit laterally, as well (lead V5 and V6). The more examples you see, the better.

The anteroseptal STEMI ECG example below is good enough to call a tombstone in lead V3. There is no lateral involvement here.
Anterior MI Pattern – Typical ST Segment Elevation
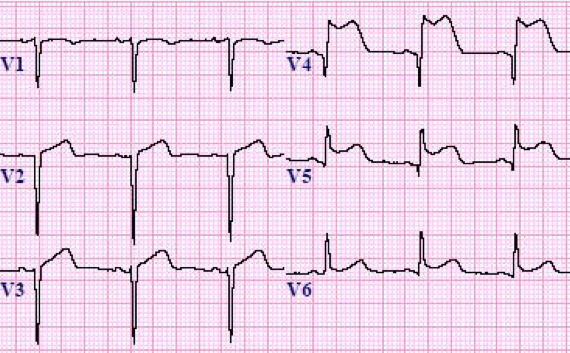
Although not quite a tombstone, there is still significant ST segment elevation here. The ST segment elevation barely reaches 5 mm in V3, and there is a bit of ST segment elevation laterally in lead V5 and V6. Thus, this example is an anterior STEMI with a little lateral involvement — no tombstones here. The ST segment in V3 is a good example of ST segment elevation that is “concave upward;” this is unlike the previous examples, where it is “concave downward” — also called “coving” of the ST segment.
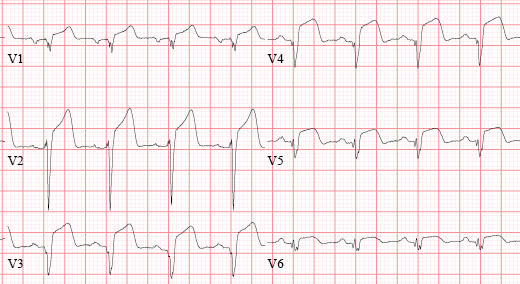
The next example below is trying to tombstone — and maybe did in lead V4. There is definite elevation of the J point in V2 to V6, at least, and minimal elevation in V1 and V6. This is a good example to quickly point out something else. Say all the precordial leads (V1-V6) looked like the minimal ST segment/J point elevation in lead V1 and V6 below — not technically 1 mm, but looks abnormal, right? If that were the case, a non-STEMI or unstable angina may be present, as the changes are indeed from myocardial ischemia, but not officially a STEMI — meaning a big time difference in regards to treatment.
Anterior MI Example – Isolated J Point Elevation
Sure, all of these anterior MIs technically have J point elevation, and we already know that the actual definition of a STEMI from the ACC/AHA is based on the J point. However, as you can see, sometimes it is quite obvious that an anterior STEMI is present, and sometimes it is not. Below is an example where there is J point elevation, but it does not quite tombstone and does not really have eye-catching ST segment elevation.

This pattern is less common during an acute MI. But again, a STEMI is a STEMI is a STEMI, and you don’t want to miss any. There are only a few times that I recall isolated J point elevation that looks more like early repolarization but really occurred during acute chest pain from an anterior STEMI. It is important to compare to an old ECG if available. If the ST segment and J point were previously normal, then an anterior STEMI should be suspected — even if only the J point is elevated in the correct clinical setting such as acute chest pain. Here are some examples of what isolated J point elevation looks like.
If you looked quickly, you may miss this one. Again, it’s not dramatic, but the J point in lead V3 is up almost 3 mm from the baseline, and maybe 2mm in lead V4. Everything else looks fine. There is no septal or lateral involvement here, which is a bit unusual. This patient had an acute mid-LAD thrombus after the septal branches and after the first major diagonal branch.
This example below actually does not meet criteria for an anterior MI based on the J point in V3 or V4, but it does in the septal leads V1 and V2. Note that even though there is barely ST segment elevation in the high lateral leads (I and aVL), there is some good reciprocal depression in the inferior leads.
دیدگاه خود را بنویسید